

Educational content — not medical advice. If you suspect chronic exertional compartment syndrome or any persistent forearm condition, please talk to a qualified doctor, ideally one familiar with athletes.
For years, I rode through it. Forearms that turned to stone three laps into a moto. Hands that wouldn't close, fingers that wouldn't release the clutch, a death grip on the bars that wasn't a choice — my body just locked up. Arm pump nearly ended my career.
In 2017, I had the surgery. The standard motocross answer to a problem most riders treat as inevitable. And for a while, it worked. But here's what I didn't know then: the surgery solved a symptom, not the root cause. The technique mistakes that were grinding my forearms into pulp in the first place were still there — and they would have caught up with me again.
Today's riders have better options than I did. After coaching thousands of riders through The Moto Academy, I've watched dozens of them fix what they thought was a medical condition with nothing more than technique work. The science around arm pump has moved on, the way the best riders in the world position their bodies on the bike has evolved, and the answer for most riders is no longer the operating table. This article is the roadmap I wish I'd had before I went under the knife.
What Arm Pump Actually Is
Most riders use "arm pump" as a catch-all term, but the medical name is chronic exertional compartment syndrome (CECS). Here's what's happening physically: when you grip the bars too tight for too long, blood floods into your forearm muscles faster than the fascia surrounding those muscles can stretch to accommodate. Pressure builds inside the compartment, blood flow gets choked off, the muscles starve for oxygen — and your hands stop working.
That's the version doctors see. But for riders, the warning signs are simpler:
- Forearms get tight and painful within 3–5 minutes of riding hard
- Grip weakens to the point you can't pull the clutch or work the front brake
- Symptoms disappear within 10–15 minutes of stopping
- It comes back as soon as you ride hard again
Severe cases can affect any rider at any level. But here's the part most riders don't hear: not every case is severe. Many "arm pump" complaints are technique problems wearing a medical disguise. Knowing the difference is the first step toward fixing it.
What It Felt Like Then
By the time I was deep in my career, arm pump wasn't a moment — it was the whole moto. I'd get to lap two with hands so locked I could barely pull the clutch in. By lap four, I was riding off the bike, not on it. My corner entries got sloppy because I couldn't feather the front brake. My jumps got dangerous because I couldn't trust my grip on the bars.
It wasn't lack of fitness. I trained harder than most pros. It wasn't lack of grip strength either — gripping harder was actually making it worse, though I didn't understand why yet. It was a body fighting itself, and the only fix anyone talked about was surgery.
I want to be clear: I'm not anti-surgery. The fasciotomy procedure — what's technically called a compartment release — is a legitimate medical option. For some riders, it's the right call. But what I'd give to go back and try the technique-first approach before I ever met the surgeon's table.
Why the Pros Are Talking About It Now
Arm pump isn't just an amateur problem. Some of the biggest names in motorcycle racing have publicly had compartment release surgery — including Pol Espargaró, who underwent the procedure during the 2021 MotoGP season and spoke openly about how it affected his racing. Multiple AMA Pro Motocross and Supercross riders have had the same surgery. It's common enough in MotoGP that paddock commentators barely flinch when a rider announces it before a race.
But here's what's changed in the last five years: the conversation around why it happens has shifted. Top motocross coaches — and a growing number of riders coming up through structured training programs — are arguing that most pre-surgery arm pump is technique-driven. The body position, grip pressure, and breathing patterns that elite riders use today are different from what was being taught a decade ago. The riders who learn those patterns early often never develop the kind of arm pump that drove riders like me to surgery.
That's the same idea behind every kid who comes through one of our 5-Day Motocross Camps learning to ride with a relaxed grip and proper attack position from day one. They're being trained out of the habits that build arm pump before those habits ever take root.
How Modern Riders Avoid Arm Pump
Watch today's Pro Motocross 250 class. Then watch a tape from 15 years ago. What stands out about today's pros is how they look on the bike: fluid and loose. Hips drive the turn instead of arms, shoulders stay relaxed, and the hands stay light on the bars except for the split-second of input.
I see the same shift in our app community and in the riders who come through TMA's 1-Day Classes. The ones who arrive with arm pump complaints almost always have the same posture problem: they're using their arms to hold themselves on the bike. Once they learn to drive grip with their core, hips, and legs — and let their hands be hands again — the pump fades.
This isn't a guarantee. Some riders have severe CECS that won't respond to technique work. But for the majority? Arm pump is a body-position problem that shows up in the forearms because that's where the load lands.
Why Technique Beats Force
Here's the counterintuitive truth almost no rider believes the first time they hear it: gripping harder makes arm pump worse, not better. When you squeeze the bars, you're constantly engaging the same flexor muscles in your forearm. They never get a break. Blood floods in, pressure builds, the cycle starts.
The riders who don't get arm pump aren't stronger. They're more efficient. They:
- Grip with the minimum pressure needed to control the bike — most of the time, that's far less than you think
- Stand up over the rough sections so their legs absorb the hits instead of their arms
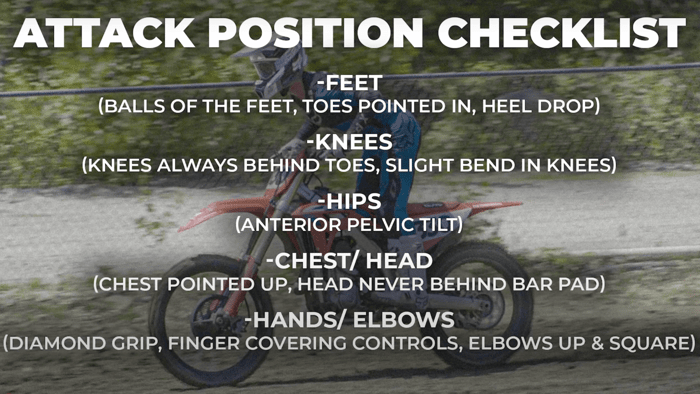
- Use the attack position (knees bent, chest forward, weight balanced) so they're not pulling themselves onto the bike with their arms
- Breathe deliberately — even mid-moto — to keep oxygen flowing through every muscle group
- Trust their grip endurance instead of training grip strength (more on this below)
None of this is exotic. Every one of these is something we drill at TMA camps and 1-Day Classes. But riders rarely figure it out on their own, because every instinct under fatigue says "grip harder." Coaching is how you re-train that instinct.
What the Science Actually Shows
Medical literature on chronic exertional compartment syndrome confirms what most experienced coaches already know: forearm compartment pressure spikes with sustained, high-tension grip. Studies in athletes across motorsports, climbing, and cycling have measured these pressure changes and traced them to repetitive forearm muscle activation — exactly what over-gripping the bars produces.
The surgery (fasciotomy) works by cutting the fascia surrounding the forearm compartment so it can expand under load. It's a documented procedure with measurable outcomes — for some riders, it genuinely is the right answer. But it's also irreversible, requires significant recovery time, and doesn't address the technique pattern that built the pressure in the first place. Some post-surgery riders report symptoms returning years later when they continue to grip the bars the same way.
That's the gap. Surgery treats the compartment. Technique addresses the input. For most riders, fixing the input — the grip, the body position, the breathing — relieves the symptom before it ever gets severe enough to need the procedure.
So what does the right input look like on the bike? It starts with body position.

The Core Advantage: #TMAPosition (Attack)
At The Moto Academy, the foundation of nearly every technique we teach is what we call the #TMAPosition — the attack position done right. Knees gripping the bike, chest forward over the bars, elbows up and out, hips driving the bike instead of arms. When a rider locks this in, their hands stop carrying weight. Their grip relaxes because it doesn't have a job to do beyond steering and throttle.
AJ talks about attack position constantly in his coaching videos — it's the difference between riding the bike and being on the bike. Riders who learn it early build a foundation that prevents arm pump from ever becoming chronic. Riders who learn it late — like I had to, after surgery — describe the same thing: their forearms stopped lighting up, even on moto-length rides, within weeks of fixing their position.
You can drill this on your own, but it's hard to feel the difference without someone watching you ride. That's why every 5-Day Motocross Camp opens with body position assessment on day one, and why our certified coaches on the 1-Day Class spend the first hour just on stance and grip pressure. You can't fix what you can't see.
Your Roadmap Before You Even Think Surgery
If your arm pump is bad enough to make you consider surgery, please talk to a doctor — that's a conversation worth having. But before you book the procedure, here's the five-step protocol I'd run with any rider who came to me with arm pump complaints today:
Step 1: Audit Your Grip
Most riders grip the bars at 70–80% strength when they only need about 20%. For the next ride, consciously ride with your fingers as relaxed as you can stand. Use your thumb and pinky to hold the bar; let your index and middle finger hover for the brake and clutch. If your forearm pump drops dramatically in a single session, you've found a major contributor.
Step 2: Stand Up Over the Rough
If you're sitting through whoops, ruts, or chop, your arms are taking the impact. Stand up. Let your legs and hips absorb the hits. Sitting locks your upper body in place — your arms become the suspension, and your forearms pay the price. Most riders who fix this one habit see arm pump drop within a few sessions.
Step 3: Build Grip Endurance, Not Grip Strength
This is the trap. Riders feel their grip failing, so they go to the gym and crush dead hangs and farmer carries. That builds maximum grip strength but does nothing for grip endurance — your ability to hold a light grip for 20+ minutes. Endurance training looks different: long isometric holds at low tension, forearm stretches, and exercises that train the extensor muscles (the back of your forearm) so they balance the flexors.
Step 4: Drill the #TMAPosition
The attack position has to become automatic. That means hundreds of reps, ideally with a coach or video review. A simple drill on your own: ride a familiar straightaway in attack position only, hands as loose as you can stand. Watch for the moment your shoulders rise toward your ears — that's the position breaking, and that's when your forearms start carrying weight again. Every TMA camper goes through this on day one. Adult 1-Day Class riders get it as their first hour. Until the position feels effortless, your forearms will keep doing the work your hips should be doing.
Step 5: Recover Like You Mean It
Forearms recover slowly under repeated load. Foam rolling the forearms, stretching the flexor and extensor groups, cold water on the forearms between motos at a long race day — these aren't optional add-ons. They're how riders who train every day keep their forearms from cumulatively breaking down. Riders also see results from breathing drills off the bike: slow, controlled breaths under simulated load teaches your body not to oxygen-debt mid-moto.

This protocol won't fix every case. But for most riders, six to twelve weeks of disciplined work on these five steps produces a noticeable change — sometimes a dramatic one. If you've done all five honestly and you're still locked up by lap three, then the conversation with a doctor is warranted. You'll go in with better data and a clearer picture.
How Much Does Arm Pump Surgery Cost?
Arm pump surgery (medically called a fasciotomy or compartment release) typically costs several thousand to over ten thousand dollars per arm in the United States, with significant variation by region, surgeon, and insurance coverage. Most riders who go this route need both arms done. Insurance coverage depends heavily on whether the condition is diagnosed as work-related, sports-related, or general athletic injury, and on your specific plan. Some plans cover it as medically necessary; others classify it as elective.
Recovery costs add up too. The procedure itself is outpatient for most riders, but you're typically off the bike for six to eight weeks minimum, with physical therapy on top. For racers, that's often the larger cost — lost season, lost momentum, lost race weekends.
None of this is a reason to avoid the surgery if it's medically warranted. But it's a reason to exhaust the technique-first path before you commit. If the technique work resolves your arm pump, you've avoided thousands of dollars and weeks off the bike. If it doesn't, you go into the surgery conversation with full information and a clear medical case.
When Surgery IS the Right Call
Despite everything above, surgery is genuinely the right answer for some riders. Even when surgery is the right call, working through technique first puts you on the operating table with better data and stronger habits to bring into recovery.
You should have an honest conversation with a qualified doctor — ideally one familiar with athletes — when:
- Your arm pump triggers within 60 seconds of every ride, regardless of intensity
- Symptoms persist for hours after you stop riding
- You've done sustained, honest technique work and seen no improvement
- You experience numbness, tingling, or color changes in your hands
- The condition is genuinely keeping you from training or racing at the level you need to
A doctor can run compartment pressure testing and tell you objectively whether the muscle pressure in your forearms is in the surgical range. That's information you can't get from technique work alone. If the test confirms severe CECS, surgery is a legitimate, often successful option — Pol Espargaró and many other pros are evidence of that.
The point of this article isn't to talk you out of surgery. It's to make sure that if you go that route, you've made an informed decision instead of a default one.
A New Option Worth Trying
If you've read this far, you're probably either dealing with arm pump now or watching someone you ride with deal with it. The technique-first path isn't a magic fix, and it isn't fast. It takes weeks of disciplined work, usually with a coach who can see what you can't.
That's why TMA built our programs the way we did. The 1-Day Classes are the lowest-friction entry point — one day of coaching where you can fix the highest-impact habits before they cost you a moto. The 5-Day Camp is the immersive version — five days of position work, drill repetitions, video review, and on-bike coaching with our certified coaches that locks the new habits in. If you want to test the water first, a Day Pass gets you on track with our team for a single session.
Riders who come to us specifically for arm pump complaints leave with a different relationship to the bars. Not because we've cured a medical condition — we haven't, and we don't claim to. They've learned to ride in a way that doesn't build the pressure in the first place. Imagine finishing a moto with hands that still work, rolling off the gate for moto two without dreading lap three. For most of them, that's the whole answer.
The riders who don't address position end up where I did — on a surgeon's table, weeks off the bike, with no guarantee the surgery holds when their old habits return.
If you want to see TMA's approach in practice, browse our kids and families guide for how we teach position from day one, or our group riding guide for how community accelerates the learning.
Arm pump shows up in your forearms, but the cause sits in your body position. Fix that, and you might never need the surgery I did.
Educational Disclaimer:
This article is for educational and informational purposes only. It reflects the experience of one professional motocross rider and the coaching observations of The Moto Academy team. It is not medical advice, does not constitute a diagnosis, and is not a substitute for evaluation, diagnosis, or treatment by a licensed medical professional. If you experience persistent forearm pain, numbness, weakness, or any symptom that affects your ability to ride safely, please consult a qualified physician — ideally one experienced with athletic injuries. The Moto Academy makes no representations regarding the efficacy of any technique described here for the prevention or treatment of chronic exertional compartment syndrome or any medical condition.